What is Head Molding? Caput Succedaneum in Newborns

“Why does my baby’s head look like a cone?!” New parents are often confused when their new addition’s scalp features bruising, swelling, or an odd shape. Not to worry, Caput succedaneum and head molding are incredibly common (temporary!) adjustments your baby made during birth. Let’s break down what these terms mean and why there’s usually […]
RSV Vaccine during Pregnancy | The Evidence
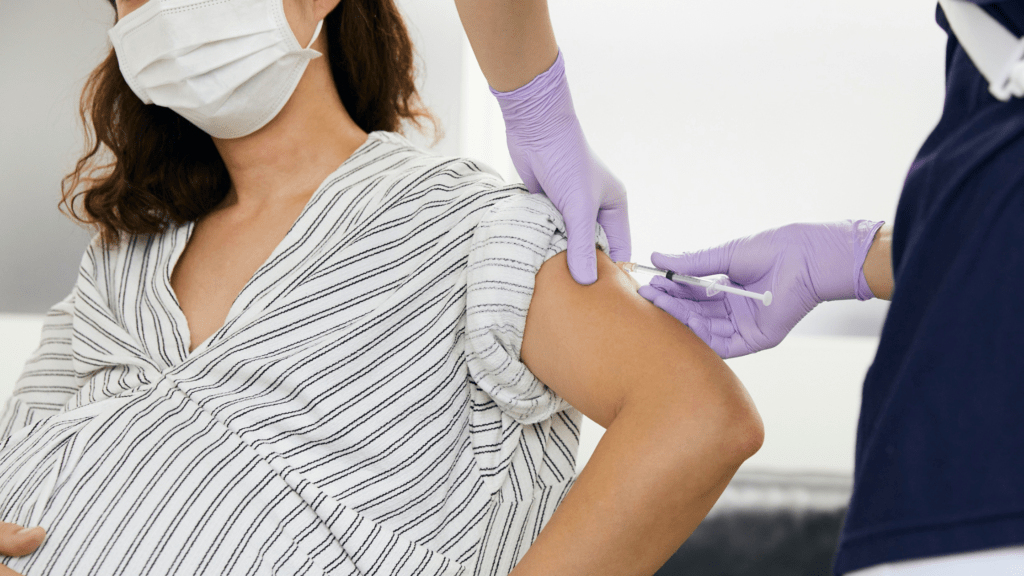
We all want to keep our newborn babies safe. When looking at common illnesses, RSV is a frequent concern amongst new parents. The latest recommendation? Recieve the RSV Vaccine during pregnancy. If your doctor has made this suggestion you may be curious how it works. Let’s take a look at what RSV is and what […]
Group B Strep: What is GBS?

If you’re pregnant it’s likely you’ve heard of Group B Strep (GBS), probably as one of the required tests for pregnant individuals. What is it and why does it matter? While GBS is common, (1 in 4 pregnant individuals have it present!) if left untreated it can pose serious health risks. Today we’re taking a […]
Birth Classes | 3 Ways Independent Curriculums Stand Out

There are pros and cons for all the birth classes on the market. Depending on what you are looking for from a class, many of the mainstream birth classes can be unappealing. You may feel like taking a childbirth series is one more thing to do before your baby arrives, but this is one thing […]
Top Positions to Try During Labor

Our top positions to try during labor? Childbirth is a process that can last a varied amount of time based on many factors. During labor, the birthing person might need to try a variety of different comfort measures. Even moving between each of these positions can help ease discomfort and be a welcome distraction. We’ve […]