3 Tips for a Healthy Third Trimester

The third trimester is between 28 and 42 weeks of pregnancy, and the final weeks before delivery. While it’s exciting to know that your baby is growing and getting ready for their birth day, you might be experiencing more discomforts. With difficulty sleeping, feeling full after a few bites, heartburn, and frequent urination, how do […]
What is Head Molding? Caput Succedaneum in Newborns

“Why does my baby’s head look like a cone?!” New parents are often confused when their new addition’s scalp features bruising, swelling, or an odd shape. Not to worry, Caput succedaneum and head molding are incredibly common (temporary!) adjustments your baby made during birth. Let’s break down what these terms mean and why there’s usually […]
Flying During Pregnancy: Air Travel Through the Trimesters

Be it for work trips or baby moons, flying during pregnancy presents a whole new world of details to consider. Walking through security and radiation exposure, the risk for increased swelling, and remaining well hydrated, are all concerns for pregnant people who use air travel at any stage of pregnancy. Here are some specific tips […]
RSV Vaccine during Pregnancy | The Evidence
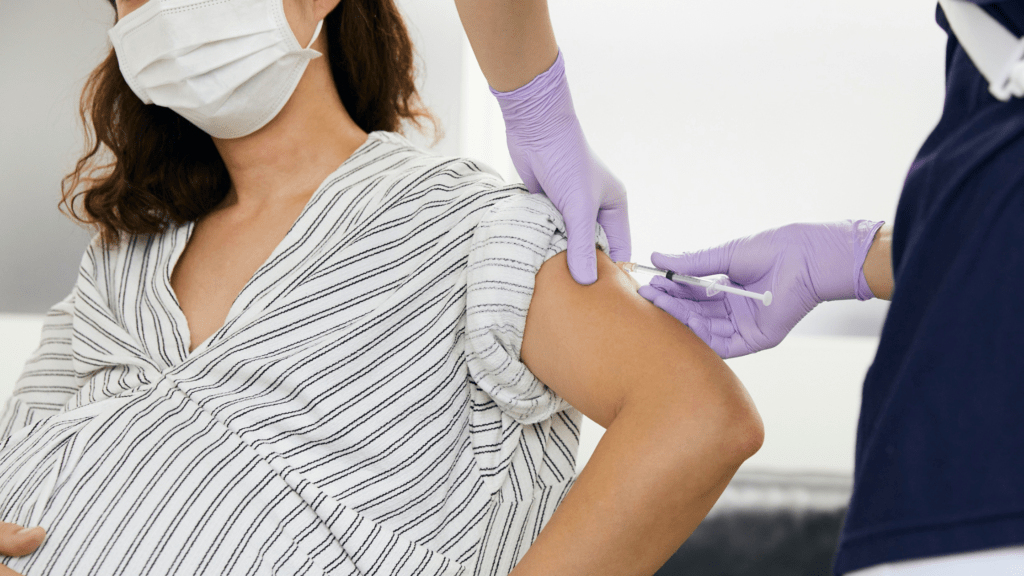
We all want to keep our newborn babies safe. When looking at common illnesses, RSV is a frequent concern amongst new parents. The latest recommendation? Recieve the RSV Vaccine during pregnancy. If your doctor has made this suggestion you may be curious how it works. Let’s take a look at what RSV is and what […]
Am I actually going into labor?

One of the most searched topics during pregnancy? “Am I actually going into labor?” Although the conventional knowledge says that pregnancy lasts nine months (which would be 36 weeks), most babies are actually born between 38 and 42 weeks. This means that you can think of your due date as more of a “due month” […]